
Abbreviation (ISO4): Chinese Journal of Alzheimer's Disease and Related Disorders
Editor in chief: Jun WANG
Chinese Journal of Alzheimer's Disease and Related Disorders >
Clinical characteristicsof cerebral amyloid angiopathy complicated by dementia in a series of 7 cases
Received date: 2019-11-19
Revised date: 2019-11-28
Online published: 2020-03-25
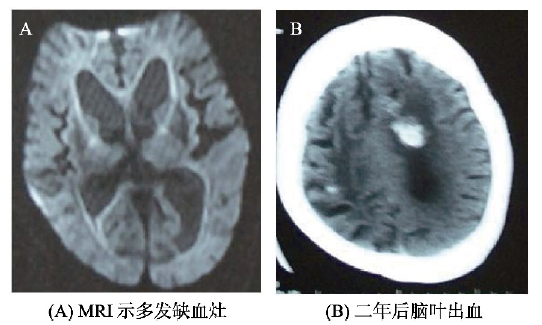
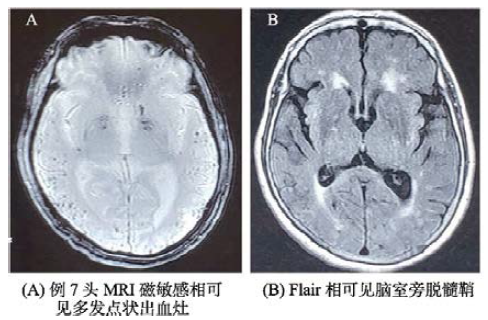
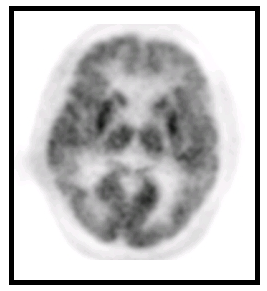
Objective: To review the clinical features at presentation in detail in outpatients with cerebral amyloid angiopathy (CAA) complicated by dementia. Methods: Seven patients were enrolled retrospectively from Department of Neurology of Peking Union Medical College Hospital were enrolled when they meet the Boston criteria. The clinical features and their CSF biomarkers and neuroimaging in detail were reviewed and analyzed. Results: There were 5 men and 2 women,and their mean age was(70.6±4.8)years old. The mean duration from memory impairment to presence of Parkinsonism was less than 1 year.Situational memory disorder,behavioral and psychiatric symptoms,and focal neurological signs were the major symptoms. MRI showed that Ventricular enlargement, white matter ischemia, white matter ischemia,and lobar hemorrhage in different patients. Neuroimage examination shows MAT grading of hippocampus I (0 case),II (2 case),III (3 case) and IV (2 case). PET showed the cingulate island sign in three patients. FDG PET showed significant lower FDG uptake in both frontal, parietal, and temporal lobe in two patients. The CSF markers (Aβ42, Aβ40, t-tau, and p-tau) have shown the same change in Alzheimer’s disease (AD) patients. The low Aβ42 content and the high t-tau and p-tau content exist in CAA patients. Conclusion: Taken together, these results suggest that dementia biomarkers might notbe useful to differentiate from AD. There is need to perform neuroimage examination on SWI to determine whether microbleeds exist in the patient with AD who have a prodigious cerebrovascular burden.
JIN Hong , GE Fangfang , ZHANG Zhenxin , LI Yanfeng . Clinical characteristicsof cerebral amyloid angiopathy complicated by dementia in a series of 7 cases[J]. Chinese Journal of Alzheimer's Disease and Related Disorders, 2020 , 3(1) : 12 -16 . DOI: 10.3969/j.issn.2096-5516.2020.01.005
表1 CAA诊断的修订BOSTON标准 |
| 1.确定的CAA(definite) | 尸检结果显示: |
|---|---|
| -脑叶、皮质或皮质下出血; | |
| -严重的淀粉样血管病变; | |
| -无其他诊断病变。 | |
| 2.病理学支持的很可能的CAA | 临床和病理(血肿抽吸或皮质活检)显示: |
| (probable) | -脑叶、皮质或皮质下出血; |
| -一定程度的淀粉样血管病变; | |
| -无其他诊断病变。 | |
| 3.很可能的CAA | 临床以及MRI和(或)CT显示: |
| (probable) | -局限于脑叶、皮质或皮质下的多发性出血灶(包括小脑出血),或局限于脑叶、皮质或皮质下的单个出血灶伴局限性(≤3个脑沟)或弥漫性(≥4个脑沟)皮质表面含铁血黄素沉积; |
| -年龄≤55岁; | |
| -无其他原因的脑出血。 | |
| 4.可能的CAA | 临床以及MRI和(或)CT显示: |
| (possible) | -单纯性脑叶、皮质或皮质下出血,或局限性(≤3个脑沟)或弥漫性(≥4个脑沟)皮质表面含铁血黄素沉积。 |
| -年龄≤55岁。 | |
| -无其他原因的脑出血。 |
表2 患者临床资料 |
| 编号 | 年龄 | 性别 | 病程 | 文化 | 起病 | 情景记忆 | 精神行为 | 定位 | 认知评估 | |
|---|---|---|---|---|---|---|---|---|---|---|
| (岁) | (年) | 程度 | 方式 | 障碍 | 症状 | 体征 | MMSE | MoCA | ||
| 1 | 74 | 男 | 5 | 高中 | 隐袭 | 有 | 无 | 无 | 11 | 7 |
| 2 | 72 | 男 | 4 | 大学 | 隐袭 | 有 | 有 | 有 | 21 | 16 |
| 3 | 69 | 男 | 2 | 大学 | 隐袭 | 有 | 有 | 有 | 26 | 12 |
| 4 | 75 | 男 | 3 | 高中 | 隐袭 | 有 | 有 | 有 | 21 | 16 |
| 5 | 83 | 女 | 2 | 大学 | 隐袭 | 有 | 有 | 无 | 22 | 14 |
| 6 | 50 | 男 | 2 | 高中 | 隐袭 | 有 | 无 | 有 | 19 | 17 |
| 7 | 71 | 女 | 3 | 初中 | 隐袭 | 有 | 无 | 无 | 17 | 14 |
表4 7例患者痴呆标志检查并与对照组比较 |
| 组别 | 例数 | Aβ42 (ng/ml) | t-tau(ng/ml) | p-tau (ng/ml) |
|---|---|---|---|---|
| CAA | 7 | 410.04 (199.23) | 350.95 (167.22) | 37.57 (24.10) |
| No-CAA | 20 | 617.78 (239.40) | 157.91 (100.99) | 24.14 (10.07) |
| P | <0.001 | <0.001 | <0.001 |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
王鲁宁, 许丹. 脑淀粉样血管病导致痴呆一例[J]. 中国卒中杂志, 2007, 2(6): 511-512.
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}