
Abbreviation (ISO4): Chinese Journal of Alzheimer's Disease and Related Disorders
Editor in chief: Jun WANG
Chinese Journal of Alzheimer's Disease and Related Disorders >
A Family with frontotemporal dementia due to MAPT gene mutation
Received date: 2021-08-02
Revised date: 2021-09-15
Online published: 2021-12-25
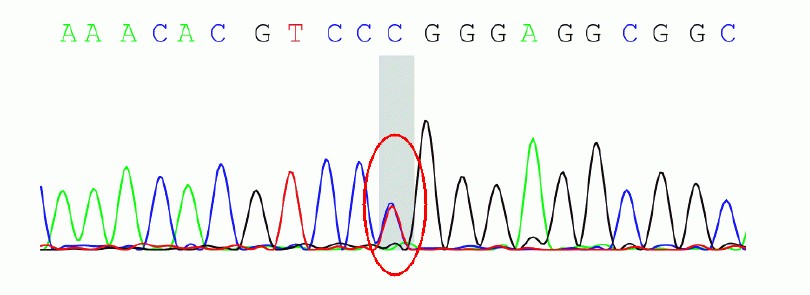
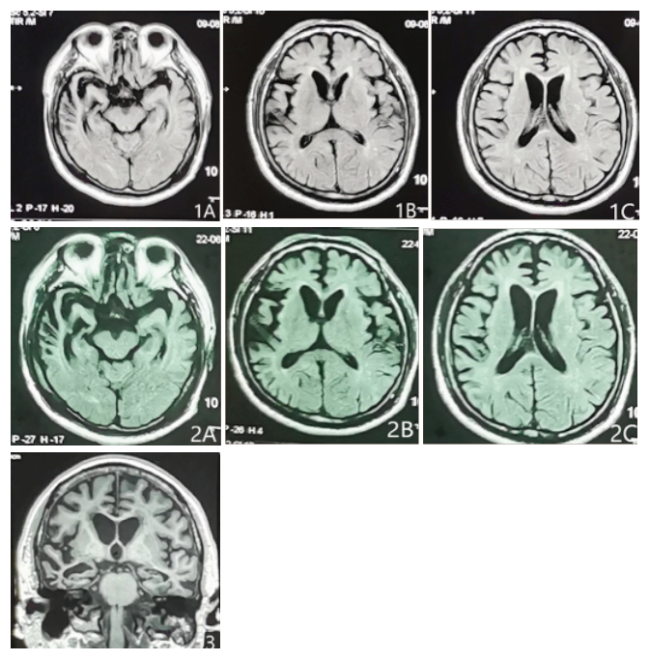
Objective: To report a family with frontotemporal dementia (FTD)due to microtubule-associated protein tau (MAPT) gene mutation diagnosed by whole exon sequencing. Methods: The family history, neuropsychological assessment, neurological examination, radiological, and genetic findings were summarized.Results: The proband is a 58-year-old male, whose father and elder sister both died due to dementia at the age of over 60. He developed the age of 56 and presented with temper change, memory loss, reckless behavior, lack of compassion, repetitive movements and overeating, without body movement symptoms. The symptoms progressed gradually and was worsened after the treatment of donepezil. Brain MRI showed atrophy involving the bi—lateral frontal and temporal lobes, specially on the right side. By whole exon sequencing.the proband was found with the c.902C>T mutation in exon 9 of the MAPT gene, at position 301 resulting amino acid proline(P)instead of leucine(L).Conclusion: This family is diagnosed as frontotemporal dementia due to MAPT gene mutation.
Key words: Frontotemporal dementia; family disease; MAPT gene
CHEN Chun-chun , ZHU Fei-qi . A Family with frontotemporal dementia due to MAPT gene mutation[J]. Chinese Journal of Alzheimer's Disease and Related Disorders, 2021 , 4(4) : 306 -309 . DOI: 10.3969/j.issn.2096-5516.2021.04.010
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
中华医学会老年医学分会老年神经病学组额颞叶变性专家. 额颞叶变性专家共识[J]. 中华神经科杂志, 2014, 47(5):351-356.
|
| [6] |
李明月, 王群. 额颞叶痴呆MAPT基因的研究进展[J]. 中华临床医师杂志(电子版), 2015(9):1679-1684.
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
Martin,
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
孙雅静. 伴有MAPT基因突变的额颞叶痴呆家系的临床特点及突变特征分析[D]. 郑州: 郑州大学, 2019.
|
| [19] |
|
| [20] |
|
/
| 〈 |
|
〉 |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}