
Abbreviation (ISO4): Acta Academiae Medicinae Sinicae
Editor in chief: Xuetao CAO
Acta Academiae Medicinae Sinicae >
Research Progress in Neurogram and Neuro-Immune Interaction of Joints in the Case of Osteoarthritis
Received date: 2023-10-09
Online published: 2024-12-03
the joints have abundant sensory nerves and sympathetic nerve fibers,which convert physical and chemical stimuli in the joints into nerve impulses that are transmitted to the central nervous system and participate in the hypersensitivity reactions of inflammatory joint diseases such as osteoarthritis(OA).This paper summarizes the distribution and functional characteristics of intra-articular nerves and focuses on the mechanism of the vagus-sympathetic autonomic circuit in regulating the immune microenvironment in joints in the case of OA.in addition,intra-articular inflammatory cytokines represented by tumor necrosis factor-αand interleukin-6 directly or indirectly induce sensory nerve action potential and activate the pain transduction pathway from the local joint to the central nervous system.the sensory nerves in the joints in the case of OA are also involved in the recruitment of immune cells and inflammatory cytokines.This neuro-immune interaction model not only provides a variety of new targets for the treatment of OA but also suggests that the treatment of OA should adopt a holistic view with comprehensive consideration of the nerve and immune microenvironment in the bone and joint and their mutual influences。
Key words: osteoarthritis; sensory nerve; autonomic nerve; inflammatory cytokines; interaction
Jian GU , Tao JIANG . Research Progress in Neurogram and Neuro-Immune Interaction of Joints in the Case of Osteoarthritis[J]. Acta Academiae Medicinae Sinicae, 2024 , 46(5) : 776 -782 . DOI: 10.3881/j.issn.1000-503X.15872
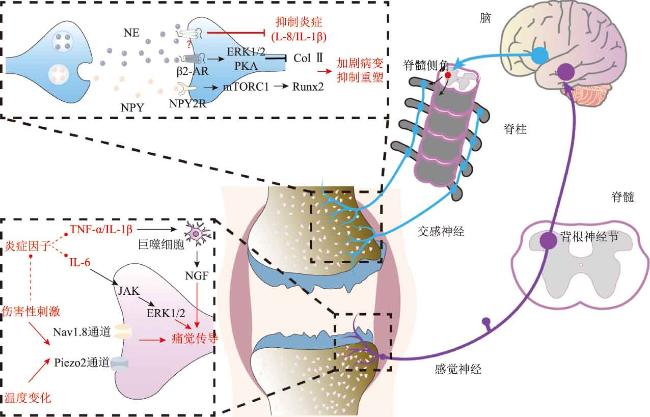
图1 骨关节炎关节内的痛觉传导通路及神经免疫互作机制NE: norepinephrine; NPY: neuropeptide Y; β2-AR: β2-adrenergic receptor; ERK: extracellular regulated protein kinase; PKA: protein kinase A; Col Ⅱ: type Ⅱ collagenase; IL: interleukin; mTORC1: mammalian target of rapamycin complex 1; JAK: Janus kinase; TNF-α: tumor necrosis factor-α; NGF: nerve growth factor |
| [1] |
|
| [2] |
|
| [3] |
|
| [4] |
|
| [5] |
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}