
Abbreviation (ISO4): Acta Academiae Medicinae Sinicae
Editor in chief: Xuetao CAO
Acta Academiae Medicinae Sinicae >
Validity and Cost-Consequence Analysis of the Brief Version of the Montreal Cognitive Assessment for Discriminating Cognitive Impairment in a Community-Based Middle-Aged and Elderly Population
Received date: 2024-06-27
Online published: 2025-07-29
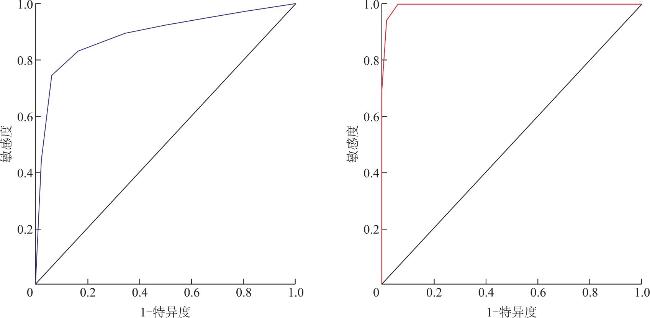
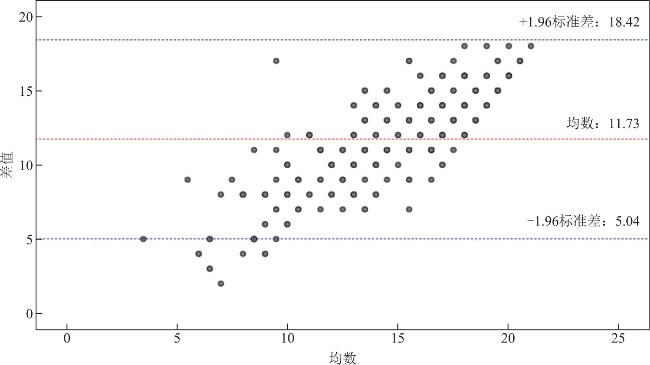
Objective To evaluate the reliability and validity and perform cost-consequence analysis of the brief version of the Montreal cognitive assessment(MoCA)for identifying cognitive impairment in a community-based population ≥50 years of age.Methods The internal consistency and retest reliability of the brief version of the MoCA were analyzed,and the area under the curve(AUC),sensitivity,and specificity were determined to discriminate mild cognitive impairment(MCI)and dementia with the clinical dementia rating(CDR)as the diagnostic criterion.The consistency between the brief version and the full version was analyzed by the Kappa test and the Bland-Altman method,and the number of individuals entering the diagnostic assessment and the overall assessment time were estimated and compared between the two versions.Results A total of 303 individuals were included in this study,of whom 192,94,and 17 had normal cognitive function,MCI,and dementia,respectively.The Cronbach’s α and re-test coefficients of the brief version of MoCA were 0.754 and 0.711(P<0.001),respectively.The brief version showed the AUC,sensitivity,and specificity of 0.889,74.5%,and 93.8% for identifying MCI,and 0.994,100%,and 93.8% for identifying dementia,respectively.When the brief version of MoCA was used to identify 94 patients with MCI in 303 individuals,107 individuals required additional diagnostic assessment,with an overall assessment time of 142.4 h,which represented decreases of 21.3% and 32.7%,respectively,compared with those of the full version.When the brief version of MoCA was used to identify 17 patients with dementia in 303 individuals,35 individuals required additional diagnostic assessment,with an overall assessment time of 70.4 h,a decrease of 29.5% in the time cost compared with the full version.Conclusions The brief version of MoCA can identify cognitively impaired individuals in a community-based middle-aged and elderly population,with diagnostic validity comparable to that of the full version but less time cost and fewer individuals needing additional diagnostic assessment to detect true-positive cases.It could be expanded for use in the community-based primary screening setting.
Ting PANG , Yaping ZHANG , Renwei CHEN , Aiju MA , Xiaoyi YU , Yiwen HUANG , Yichun LU , Xin XU . Validity and Cost-Consequence Analysis of the Brief Version of the Montreal Cognitive Assessment for Discriminating Cognitive Impairment in a Community-Based Middle-Aged and Elderly Population[J]. Acta Academiae Medicinae Sinicae, 2025 , 47(3) : 382 -389 . DOI: 10.3881/j.issn.1000-503X.16242
表1 完整版MoCA和简短版MoCA的比较 |
| Project | Full Version of MoCA | Brief MoCA |
|---|---|---|
| Total score | 30 points | 12 points |
| Evaluation time | 12~15 min | 5~8 min |
| Cognitive Domain and Scoring Method | (1) Visuospatial and executive function (5 points); (2) Naming (3 points); (3) Immediate memory (0 points); (4) Attention (6 points); (5) Language function and fluency (3 points); (6) Abstraction (2 points); (7) Delayed recall (5 points); (8) Orientation (6 points) | (1) Immediate memory (0 points): Participants are asked to recall five words immediately, no score is given; (2) Verbal fluency (1 point): Name as many animal names as possible within 1 minute, 1 point is given if ≥12 animals are named, otherwise no score; (3) Delayed recall (5 points): Participants are asked to recall the five words after a 5-minute delay, 1 point is given for each correct answer; (4) Orientation (6 points): Six orientation questions about year, month, day, weekday, city, and address are asked, 1 point is given for each correct answer. |
注:MoCA:蒙特利尔认知评估量表 |
表2 研究对象的人口学特征 |
| Feature | NCI(n=192) | MCI(n=94) | Dementia (n=17) | Total number of people (n=303) | P |
|---|---|---|---|---|---|
| Age (±s(years old) | 69.6±6.7 | 74.5±8.6 | 79.8±10.1 | 71.7±8.1 | <0.001 |
| Female[n(%)] | 146( 76.0) | 58(61.7) | 12( 70.6) | 216(71.3) | 0.042 |
| Han Chinese[n(%)] | 192(100.0) | 93(98.9) | 17(100.0) | 302(99.7) | 0.366 |
| Education leveln(%)] | <0.001 | ||||
| Primary school or below | 46( 24.0) | 57(60.6) | 14( 82.4) | 117(38.6) | |
| Junior high school | 96( 50.0) | 30(31.9) | 2( 11.8) | 128(42.2) | |
| High school or above | 50( 26.0) | 7( 7.4) | 1( 5.9) | 58(19.1) | |
| Full MoCA scoring (±s, points) | 23.2±3.6 | 16.9±4.2 | 11.7±3.7 | 20.6±5.2 | <0.001 |
| Brief Version of MoCA Score±s, points) | 10.1±1.6 | 6.9±2.0 | 4.5±1.6 | 8.8±2.5 | <0.001 |
| Orientation | 5.7±0.6 | 5.3±1.0 | 4.2±1.5 | 5.56±0.9 | <0.001 |
| Fluency of language | 0.8±0.4 | 0.5±0.5 | 0.1±0.2 | 0.7±0.5 | <0.001 |
| Memory | 3.6±1.3 | 1.1±1.5 | 0.2±0.4 | 2.6±1.9 | <0.001 |
注:NCI:无认知障碍;MCI:轻度认知障碍 |
表3 简短版MoCA判别MCI和痴呆的诊断参数 |
| Diagnostic Grouping | Area under the curve (95%CI) | Critical value (n) | Sensitivity (%) | Specificity (%) | Positive predictive value (%) | Negative Predictive Value (%) | Accuracy (%) | Accurate diagnosis of cases Proportion (n/n) | Correctly identifying healthy individuals Proportion (n/n) |
|---|---|---|---|---|---|---|---|---|---|
| MCI and NCI | 0.889(0.843-0.934) | 7/8 | 74.5 | 93.8 | 85.4 | 88.2 | 87.4 | 70/94 | 180/192 |
| Dementia and NCI | 0.994(0.987-1.002) | 7/8 | 100.0 | 93.8 | 58.6 | 100.0 | 94.3 | 17/17 | 180/192 |
| [1] |
中华医学会神经病学分会痴呆与认知障碍学组. 阿尔茨海默病源性轻度认知障碍诊疗中国专家共识2021[J]. 中华神经科杂志, 2022, 55(5):421-440.DOI:10.3760/cma.j.cn113694-20211004-00679.
|
| [2] |
卢添欢, 宇传华. 基于全球视角的中国痴呆症疾病负担现状及趋势分析[J]. 中华疾病控制杂志, 2022, 26(6):684-690.DOI:10.16462/j.cnki.zhjbkz.2022.06.012.
|
| [3] |
|
| [4] |
中华医学会神经病学分会痴呆与认知障碍学组, 中国医师协会神经内科医师分会认知障碍疾病专业委员会. 前驱期阿尔茨海默病的简易筛查中国专家共识(2023年版)[J]. 中华神经医学杂志, 2023, 22(5):433-444.DOI:10.3760/cma.j.cn115354-20230330-00191.
|
| [5] |
|
| [6] |
夏安琪, 李军, 岳玲, 等. 蒙特利尔认知评估量表在中国社区老人中的应用[J]. 上海交通大学学报(医学版), 2021, 41(12):1662-1667,1661.DOI:10.3969/j.issn.1674-8115.2021.12.017.
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
何梦霏, 王梦寰, 高婧, 等. 中文版卒中认知评估量表在非失语脑卒中患者中的信效度和临床应用[J]. 中国康复医学杂志, 2024, 39(12):1797-1803.
|
| [18] |
于文华, 李建国, 段文燕, 等. 老年人功能受损评估量表在社区老年人中的信效度检验[J]. 中国全科医学, 2024.DOI:10.12114/j.issn.1007-9572.2024.0311.
|
| [19] |
郭佳翔. 蒙特利尔认知评估量表中文版的初步应用[D]. 北京: 北京协和医学院, 2011.
|
| [20] |
张嘉祺, 马迪, 阚来弟, 等. 五分钟蒙特利尔认知评估对脑卒中患者认知筛查的研究进展[J]. 中国老年保健医学, 2018, 16(5):25-28.DOI:10.3969/j.issn.1672-2671.2018.05.005.
|
| [21] |
|
| [22] |
彭一念, 殷樱, 冯雅丽. 两种五分钟蒙特利尔认知评估方案评估脑卒中患者的对比研究[J]. 重庆医科大学学报, 2020, 45(10):1497-1500.DOI:10.13406/j.cnki.cyxb.002634.
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
李晗, 李霞. 老年人认知障碍的智能化认知筛查工具研究进展[J]. 中国医学科学院学报, 2024, 46(1):104-110.DOI:10.3881/j.issn.1000-503X.15519.
|
| [32] |
|
| [33] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}