
Progress in the Study of Exhaled Gas Fingerprinting in Diabetes
Received date: 2023-11-08
Revised date: 2024-02-29
Online published: 2024-05-30
Supported by
National Key Research and Development Program of China(2018YFA0208504)
Shanghai "Science and Technology Innovation Action Plan" Medical Innovation Research Special Program(22Y11900600)
General project of the National Natural Science Foundation of China(8217142522)
in recent years,there has been a significant surge of interest in exploring exhaled gas detection within the context of diabetes research.This burgeoning field has attracted considerable attention due to its potential implications for the early detection and management of diabetes mellitus.Through a comprehensive synthesis of 114 pertinent scholarly works,researchers have delved into the intricate association between diabetes mellitus and exhaled gas detection.Leveraging state-of-the-art detection and analysis methodologies,including gas chromatography,mass spectrometry,spectroscopy,and sensor-based detection systems.This review provides an overview of the composition of some volatile organic compounds and their sources in the exhaled gas of diabetic patients.Furthermore,the application of machine learning-based algorithms has been scrutinized for its potential to facilitate predictive modeling of diabetes risk and associated complications.This comprehensive review also examines the national and international landscape of the development and application of exhaled gas detection methodologies in diabetes research,offering critical insights into current limitations and potential avenues for future research and application。
1 Introduction
2 Components and sources of exhaled gas in diabetes
2.1 Composition of exhaled gas
2.2 Causes of changes in the composition of exhaled gas and its physiological origin in diabetic patients
3 Diabetic exhaled gas detection method
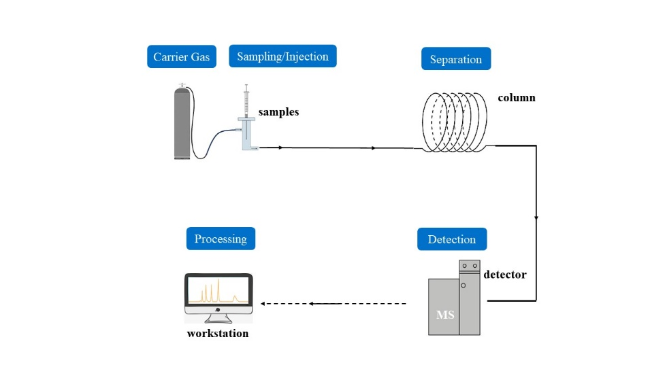
3.1 Gas chromatography detection methods
3.2 Direct detection by mass spectrometry
3.3 Spectroscopic detection methods
3.4 Sensor Detection Methods
4 Diabetes exhaled gas detection algorithm
5 Conclusion and outlook

Wu Haoping , Li Lei , Zeng Rui , Zhu Yuchen , Zhao Bin , Feng Fei . Progress in the Study of Exhaled Gas Fingerprinting in Diabetes[J]. Progress in Chemistry, 2024 , 36(4) : 601 -611 . DOI: 10.7536/PC231110
表1 Potential biomarkers of exhaled breath in diabetes[20,25,26,29,32,36]Table 1 Exhaled breath potential biomarkers of diabetes[20,25,26,29,32,36] |
| Marker name | Source/Association with diabetes |
|---|---|
| Acetone | Excessive breakdown of fat and increased concentration of ketone bodies in the blood. |
| Isopropyl alcohol | Acetone reduction produces. |
| Potassium nitrate | The appearance of hyperoxidation in the body and an increase in the concentration of ketone bodies in the blood. |
| Isoprene | Lipid peroxidation process related. |
| 8-isoprostane | It is the end product of unsaturated fatty acid lipid peroxidation (non-enzymatic reaction) catalyzed by free radicals, and its production is closely related to oxidative stress damage in the body. |
表3 Comparison of Exhaled Gas Detection Methods in Diabetes Mellitus[41,43⇓~45,65,91,104]Table 3 Comparison of diabetic exhaled gas detection methods[41,43⇓~45,65,91,104] |
| Methods of analysis | Vantage | Drawbacks |
|---|---|---|
| GC/GC-MS | 1. Good ability to recognize compounds. 2. High sensitivity. 3. High accuracy. | 1. Requires sample preparation. 2. Requires pre-concentration. |
| SIFT-MS | 1. High sensitivity. 2. Low detection limit. 3. Fast Response. | 1. Unrecognizable compound. |
| PTR-MS | 1. High sensitivity. 2. No pre-concentration. 3. No sample collection required. 4. Strong resistance to environmental factors. | 1. Unrecognizable compound. 2. The detection range is narrow |
| Spectroscopic methods | 1. Real-time detection of low concentration compound molecules. 2. High resolution. 3. High selectivity. | 1. Poor ability to detect multiple compounds simultaneously. |
| E-nose | 1. Low cost. 2. Small size. 3. Easy to operate. | 1. Cannot screen for multiple diseases. 2. Due to the influence of water vapor in the analyte, a single compound in the complex gas mixture cannot be identified. |
表4 Diabetes exhaled breath detection algorithm[105,106,108⇓⇓ ~111]Table 4 Diabetes exhaled gas detection algorithm[105,106,108~111] |
| Algorithm | Vantage | Drawbacks |
|---|---|---|
| SVM | 1. High efficiency. 2. Strong generalization ability. 3. Suitable for complex data sets. | 1. Not applicable to multiple classification problems. 2. Sensitive to missing data. |
| CNN | 1. Automatic feature extraction. 2. Hierarchical feature learning. | 1. Risk of overfitting. |
| [1] |
|
| [2] |
|
| [3] |
Diabetes Branch of Chinese Medical Association. Chinese Journal of Practical Internal Medicine, 2021, 41(8): 668.
( 中华医学会糖尿病学分会. 中国实用内科杂志, 2021, 41(8): 668.)
|
| [4] |
( 刘丽华, 欧阳璐, 李舒梅. 赣南医学院学报, 2014, 34(6): 978.)
|
| [5] |
( 李志坚, 李言飞, 孙勇. 医学理论与实践, 2011, 24(19): 2352.)
|
| [6] |
|
| [7] |
|
| [8] |
|
| [9] |
|
| [10] |
|
| [11] |
|
| [12] |
|
| [13] |
|
| [14] |
|
| [15] |
|
| [16] |
|
| [17] |
|
| [18] |
|
| [19] |
|
| [20] |
|
| [21] |
|
| [22] |
|
| [23] |
|
| [24] |
|
| [25] |
|
| [26] |
|
| [27] |
|
| [28] |
|
| [29] |
|
| [30] |
|
| [31] |
|
| [32] |
( 唐丹, 张剑彬, 陈莉, 段雪莲. 重庆医学, 2018, 47(17): 2369.)
|
| [33] |
|
| [34] |
|
| [35] |
|
| [36] |
|
| [37] |
|
| [38] |
|
| [39] |
|
| [40] |
|
| [41] |
|
| [42] |
|
| [43] |
|
| [44] |
|
| [45] |
|
| [46] |
|
| [47] |
|
| [48] |
|
| [49] |
|
| [50] |
|
| [51] |
|
| [52] |
|
| [53] |
|
| [54] |
( 李雯雯, 段忆翔. 化学进展, 2015, 27(4): 321.)
|
| [55] |
|
| [56] |
|
| [57] |
|
| [58] |
|
| [59] |
|
| [60] |
|
| [61] |
|
| [62] |
|
| [63] |
|
| [64] |
|
| [65] |
|
| [66] |
Hengerics Szabó A,
|
| [67] |
|
| [68] |
|
| [69] |
|
| [70] |
|
| [71] |
|
| [72] |
Zeki Ö C,
|
| [73] |
|
| [74] |
|
| [75] |
|
| [76] |
|
| [77] |
|
| [78] |
|
| [79] |
|
| [80] |
|
| [81] |
|
| [82] |
|
| [83] |
|
| [84] |
|
| [85] |
|
| [86] |
|
| [87] |
|
| [88] |
|
| [89] |
|
| [90] |
|
| [91] |
|
| [92] |
|
| [93] |
|
| [94] |
|
| [95] |
|
| [96] |
|
| [97] |
|
| [98] |
|
| [99] |
|
| [100] |
|
| [101] |
|
| [102] |
|
| [103] |
|
| [104] |
|
| [105] |
|
| [106] |
|
| [107] |
|
| [108] |
|
| [109] |
|
| [110] |
|
| [111] |
|
| [112] |
|
| [113] |
|
| [114] |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}